MEDICAL UNIT ACTIVITIES
Alert and Movement
The professional medical personnel who served in the Dominican Republic during the combat phase of the operation were generally inexperienced in combat and in the handling of battle casualties, but had gone through repeated alert and practice situations. When the Dominican alert came in late April, those in ready force status prepared men and equipment for airdrop or air-land operations in accordance with contingency operations planning.
For example, Company D (commanded by CPT Robert F. Elliott, MSC) of the 307th Medical Battalion had assumed normal division ready force posture in support of the 3d Brigade at noon on 23 April. This meant that 16 medical personnel and equipment were prepared for parachute operations, while 23 personnel, six ambulances, one 1/4-ton truck, one 3/4-ton truck, one 3/4-ton trailer, one 2 1/2-ton truck, and one 1 1/2-ton water trailer were prepared for air-land operations, as prescribed by standing operating procedures and policies dictated by higher echelons. Thus when the 3d Brigade alerted the company to a higher status of readiness at 0030 on 26 April, all personnel were assembled in short order. The next higher stage of alert before actual takeoff came at 1800 on 28 April, and all personnel and equipment were available within an hour. At 1430 the next day the parachute element was split, with an officer in charge of each element, and lodged with the 505th Airborne Infantry Battalion and with the 508th Airborne Infantry Battalion for outloading. At approximately 1730 the same day, the air-land element moved by convoy from Fort Bragg to Seymour-Johnson Air Force Base, N.C. Upon arrival they moved immediately to the marshaling area to await loading into C-124 transport aircraft. There, as planned, the Company D personnel took on an orthopedic surgical team, the 139th Medical Detachment (KB) from Valley Forge (commanded by MAJ John B. McGinty, MC), which had arrived at 1230 the same day.32
28
The orthopedic surgical team, which was officially attached to Company D until it could join the 15th Field Hospital, was the first unit loaded out at Seymour-Johnson Air Force Base. After taking off at 0100 on 30 April and making a stop at Pope Air Force Base, it arrived at San Isidro at 0645. At San Isidro the team secured (with the cooperation of the Dominican Air Force) the use of a Technical Instruction Building near the south end of the runway. The building then served as Company D clearing station during the next 30 hours.
Throughout the night and morning of 29-30 April, the air-land and parachute elements of Company D (which also air-landed) assembled at the Technical Instruction Building. Equipment was de-rigged and hand-carried to the site by medical personnel, as was a large amount of automatic issue medical supplies which had been flown in from Puerto Rico for the operation.
CPT Leon R. Moore, ANC, began organizing the clearing station, and it was in full operational status before 1600 on 30 April. Only one Army battle casualty arrived before the clearing station was fully set up and he was evacuated to the USS Boxer after emergency treatment for a bullet wound.
While in the Technical Instruction Building the professional staff of Company D alternated duties with the staff of the orthopedic surgical team.
Company D frontline ambulances were dispatched to a battalion aid station, which had been set up at the Duarte bridge, and evacuated t8 battle casualties to the clearing station during the next 24-hour period. Ambulance drivers came under fire to perform their duties.
At about 1530 on 30 April, the Airborne medical personnel sent various medical supplies via Marine helicopter to the Marine aid station which was operating near the Embajador Hotel.
During the evening of 30 April and the following morning, the Division Surgeon, elements of the 584th Ambulance Company, and the 15th Field Hospital, as well as Company C of the 307th Medical Battalion, arrived at the Technical Instruction Building, which was the objective area. In the days immediately following, the rest of the 307th Medical Battalion and the various Battalion aid stations were flown in. The departure of Medical Battalion personnel from North Carolina occurred as follows:
29
| Deployed 29 April | Officers | Enlisted men |
|---|---|---|
| Headquarters and Company A | 3 | 0 |
| Company C | 1 | 0 |
| Company D | 1 | 25 |
| Deployed 30 April | Officers | Enlisted men |
|---|---|---|
| Headquarters and Company A | 5 | 0 |
| Company B | 1 | 0 |
| Company C | 2 | 47 |
| Company D | 1 | 27 |
| Deployed 1 May | Officers | Enlisted men |
|---|---|---|
| Headquarters and Company A | 1 | 2 |
| Deployed 3 May | Officers | Enlisted men |
|---|---|---|
| Headquarters and Company A | 2 | 0 |
| Company B | 2 | 46 |
| Deployed 4 May | Officers | Enlisted men |
|---|---|---|
| Headquarters and Company A | 5 | 17 |
| Deployed 5 May | Officers | Enlisted men |
|---|---|---|
| Company B | 3 STRAC Designee Medical Corps officers from outside the Division | 0 |
| Deployed 6 May | Officers | Enlisted men |
|---|---|---|
| Company C | 1 | 0 |
Company A was not actually deployed as the information above would indicate. The enlisted men listed as deploying with "Headquarters and Company A" were part of the Battalion Headquarters staff, while the officers listed after "Headquarters and Company A" actually were the medical professional staff of the Battalion, redistributed after reaching DOMREP. Part of the Battalion Headquarters and all of Company A remained at Fort Bragg. The total number of 307th Medical Battalion personnel deployed from North Carolina from 29 April to 6 May, was 28 officers and 164 enlisted men.
30
The alert and movement was not as smooth for all units as it was for Company D. Although the medical support for the DOMREP operation was adequate and effective throughout, confusion accompanied rushed operations. And in the Dominican crisis, information was not always disseminated to those with a need to know as fast as it should have been.
For example, Company C of the 307th Medical Battalion was not on ready force status when it was alerted at 2230 on 28 April.33 Required equipment was on hand and personnel were assembled in an hour and a quarter, but they received no definitive briefing at that time and the possibility of quick deployment seemed remote.
The following day, officers of Company C were briefed at Battalion Headquarters and learned that Company D was being prepared for movement in support of the 3d Brigade. It was late afternoon before it was determined that Company C would be deployed to support the entire 2d Brigade rather than just part of it or as support for the Division as a whole. Later that night the company loaded all its equipment on trucks.
Then the next morning (30 April) at 0400 the unit was alerted for movement and its officers told that the company would be under Division rather than Brigade control. Later that morning personnel were paid, ate, and then loading began. The planes took off at 1330. During the flight it was found that not enough in-flight rations had been issued for the entire company, but the 4-hour flight had begun shortly after lunch and additions rations were not really needed. By 1845 Company C and almost all of its equipment were at San Isidro.
After they arrived in the Dominican Republic, Company C officers found that they had no specific instructions on whom they should report to or on what was to be done. So, after unloading the aircraft they held the unit in one location. When they heard that Company D was in a building near the end of the runway, they contacted them, left some needed equipment, and awaited further instructions.
The following day, 1 May, personnel were briefed on the tactical and medical situation, including their potential role in the medical support operation, and were told that there was a water shortage. Then, in the afternoon, the Company C commander accompanied the Division Surgeon in quest of a place to set up. It was decided that the company should move in near 3d Brigade Headquarters on the edge of Santo Domingo and provide support in order to conserve time and effort and to avoid further confusion,
31
even though Company D had originally been slated to provide such support. Therefore Company C moved and began to treat and evacuate patients.
Had the original plan been followed, Company D, already housed in the Technical Institute Building, would have had to move out and reload their equipment, whereas Company C was still "on wheels" and more easily deployable. Movement of Company D would also have interrupted the only existing Army medical support available at that time.
Meanwhile, the 15th Field Hospital and other support units had been having their problems. After the 5th Logistical Command received a preliminary alert notification on 27 April, the 55th Medical Group was placed on a higher alert status on 29 April. A series of conferences and exchanges of information had begun and finally resulted in the listing of medical units actually to be used in the Dominican operation (p. 7). At 0510 on 30 April, the 55th Medical Group had been informed that one (100-bed) hospital unit of the 15th Field Hospital was to "move out immediately." Twenty minutes later it was learned the entire field hospital was to go to the Dominican Republic as quickly as feasible.34
Hospital personnel began loading equipment and one hospital unit was ready to go before noon. Planes carrying the first hospital unit took off throughout the afternoon and into the night.35
The next morning, 1 May, elements of the hospital unit (and the first platoon of the 584th Ambulance Company [-]) began arriving at San Isidro approximately 12 hours ahead of some necessary equipment. There had been a mixup in the loading line at Pope Air Force Base, and a detour to Puerto Rico with some of the personnel scheduled to go to Santo Domingo.36 LTC William L. Richardson, MC, the hospital commander, reported to the 82d Division Headquarters at San Isidro, and although the Division had many activities in progress, the Division Surgeon, MAJ Quitman W. Jones, had Company D move out of the Technical Instruction Building at the airfield so that part of the hospital unit could begin setting up there. The orthopedic surgical detachment (139th of Valley Forge) was detached from Company D and attached to the hospital.
32
Before the hospital unit was completely unpacked, however, personnel had to find a new place for two bodies which had been left in the operating room. Arrangements were finally made with the Air Force to keep the bodies in an appropriate place for handling by a small Graves Registration Unit which had just arrived.
The 15th Field Hospital then set up a 20-bed ward, operating room, central materiel section, pre-operative and receiving sections, laboratory, X-ray, and pharmacy. Several casualties with gunshot wounds were treated and evacuated almost immediately. The patient load on 1 May was 16 and this number increased daily for the next several days.
Back at Fort Bragg the remaining hospital units and headquarters element of the 15th Field Hospital encountered numerous packing and transportation problems. However, they and the 53d Medical Detachment (General Surgical) and another platoon of the 584th Ambulance Company were able to join the first hospital unit of the 15th at San Isidro over the next 2-day period.
Buildup and Operations
The most significant military casualties of the operation were received during the first few days of conflict and in mid-June. Disposition of these casualties was described in the section, "Extent of Medico-Military Operations" (p. 14).
The medical battalion provided direct support to the 82d Airborne Division's combat brigades from the beginning of the operation until 5 May, when each company reverted to battalion control. Then the medical companies provided support by area.
A series of leapfrog movements by the medical units characterized the first few days of the operation. Company D of the 307th Medical Battalion vacated the Technical Instruction Building at San Isidro on 1 May to make room for the 15th Field Hospital. Since Company C37 was then supporting the 3d Brigade, Company D went into mobile reserve until the next day when it began supporting the 2d Brigade. Meanwhile Company D ambulances and professional staff augmented Company C operations.
On 3 May, Company D moved 14 of its men and four vehicles through Santo Domingo in support of the 2d Brigade as it opened up the corridor (map 4). After getting into the corridor, the Company D commander, CPT
33
Elliott, received orders to begin a civic action mission. He received permission from the Mother Superior, Sor Maria Auxiliadora, Salesian Sisters, to locate a clearing station in Colegio Maria Auxiliadora on San Juan Bosco Street. At that time the corridor boundary was the rear wall of the school and firing was heavy in the area. (A battalion aid station was located directly opposite in Colegio San Juan Bosco.) The rest of Company D remained "on wheels" near Company C for a short time, then the whole of Company D was established at the school, where it maintained its base until redeployment in July.
34
Also on 3 May, the 15th Field Hospital, dissatisfied with its location, moved closer to the city. A surgical team and two hospital wards were moved forward to the area where Company C was set up, about half a mile from Duarte bridge. Later in the day the entire hospital was ordered to the forward location, and when it became operational, most of the flow of combat patients was directed into the field hospital. The 15th was to begin admitting civilian patients at the same time.
Company C had also been directed to begin civic action and its mobile aid team was receiving civilian patients. The company moved in toto to a schoolhouse in town to set up a clearing station ahead of the field hospital, but immediately came under heavy fire and was pulled back. In this action one medic was wounded. On 5 May, Company C set up a clearing station under the Duarte bridge while its mobile aid station went back into the city each day.38
Company B of the 307th Medical Battalion arrived at San Isidro on 4 May to provide medical support to the 1st Brigade of the 82d Airborne Division.39 After establishing in a temporary location during its first two days on the island, the medical company reverted to Battalion control and was positioned adjacent to the Support Command Headquarters near the 82d Division's Command Post at the Military Academy, where it maintained its facilities until November, when it was redeployed to Fort Bragg. While there, Company B provided division-level medical service to the division rear area and unit level medical service for rear elements of the division with no organic medical capability.
After a number of moves to provide area and direct Brigade support, Company C finally found a "permanent" home at Camp Randall in the fairgrounds area near the Hotel Embajador. Not all of the Company's property was ever moved to the Dominican Republic, but at the end of the year it was operating at full personnel strength with a dental, surgical, and holding capability, and with some extra equipment left by Company B.
Throughout their stays in the Dominican Republic, the medical companies operated on a flexible base. They administered mobile aid stations, civilian aid stations at various locations, provided medical service to the Division's troops, and relieved each other at various facilities throughout the city and nearby countryside area.
The 15th Field Hospital and its associated units were not quite so mobile, but they moved a lot. On 3 May, the 15th had displaced Company
35
C at a location east of Santo Domingo. This particular area, rocky and overgrown, was also subject to the adverse effects of weather. The ground became mud when it rained, and the rainy season soon started (fig. 4).40
Meanwhile the 714th Preventive Medicine Detachment and the 69th Medical Detachment (Veterinary Food Inspection) had arrived on the scene, were attached to the 15th Field Hospital, and began their missions as previously described. (The 69th was located at the port of Jaina most of the time, with the responsibility of inspecting all foodstuffs used by the Inter-American Peace Force.) The 545th Medical Detachment (Supply) arrived in toto at San Isidro on 1 May, on which date MAJ Daniel S. Goolsbee, MSC, assumed command.41
36
On 8 May the unit was attached to the 16th Quartermaster Battalion and 3 days later moved to the Boca Chica-Andrés area, where it occupied part of a sugar warehouse. On 11 June the supply unit moved back with the 15th Field Hospital and stayed attached to it until December.
"The 545th Medical Detachment (Supply) provided the only facilities for receiving, storing, and issuing of medical supplies on the island. Support was given to all units located on the island who maintained any type of medical mission. This included the 82d Airborne Division, Special Forces, 15th Field Hospital, Brazilian and Honduran units, and the Navy and Marines located off coast."42
During the year more than 6,000 line items were requisitioned by the unit while in the Dominican Republic.
The 54th Medical Detachment (Helicopter-Ambulance) of Fort Benning, Gal, was first alerted for possible movement on 2 May. There followed a period of intense confusion among personnel over where the unit would go, how it was to go, and what type helicopters it would use. But by the early morning hours of 3 May, unit personnel and five UH-1B helicopters from Lawson Army Airfield were assembled at Mayport Naval Air Station. Two and one-half days after boarding the USS Boxer, the helicopter outfit, with CPT Kent E. Gandy, MSC, 43 in command, was offshore from Santo Domingo on the morning of 6 May.44 The aviators flew their craft from the ship directly to San Isidro while land vehicles and supplies were put ashore at Jaina. The motor convoy traveled from Jaina through the city in early darkness and came under fire immediately, but made it to the airport without casualties.
Before the number of helicopters in the unit was reduced from five to two, some of them were stationed for short periods with the Marines on the west side of Santo Domingo, at the Naval offloading site at Andrés, 20 miles east of the city, and elsewhere when needed. Usually two aircraft were kept in the vicinity of the field hospital, to which the helicopter unit was administratively attached.
37
Because of the proximity of the various medical units to the scene of combat activity, the helicopters were not used so much for emergency medical evacuation as for other purposes, such as blood and supply hauls and transport of medical personnel. Most medical evacuation flights which were made were between the field hospital and the casualty staging facility at San Isidro. By 25 October, 192 patients had been transported on 137 medical evacuation missions and there had been 18 blood runs. The unit had flown a total of 487 hours in DOMREP, but much of that time included training for pilot proficiency, since the unit had not been equipped with UH-1B aircraft before deployment to the island.
Meanwhile, back in May, the 15th Field Hospital was still in the mud. By 9 May the hospital area had become "so congested by the number of attached units" that one platoon of the ambulance company was sent to Boca Chica, where it could provide ambulance support to the Rest and Recreation area set up there.45
On 18 May the rains became heavier. The next day trucks going into the hospital area had to avoid the roads and push through the brush. The A and D tent, treatment tent, three of the five wards which were set up,46 and some other tents were "completely under water."47 The following day (20 May) permission was granted by Force Headquarters for the hospital to be moved to an airstrip about two miles from the Duarte bridge (fig. 5) where at least part of the tents would be on hard ground. One unit of the hospital had been kept loaded and in reserve, not even partially set up. This unit was moved first and set up at the new location. Throughout the operation, the full capability of the hospital was never tested, part of it being in reserve at all times until two of the three hospital units and the hospital headquarters were returned to Fort Bragg in July.48
No dietitians were assigned to the 15th Field Hospital, so the nurses (there were several female nurses from Fort Bragg and other posts with the hospital) were responsible for serving patients' meals and special
38
Figure 5.--The 15th Field Hospital relocated on an abandoned airstrip.
diets. Plastic trays and cups and stainless silverware were used. After the first few weeks, C-rations were supplemented with and later supplanted by B-rations. Even at its location at the airstrip, PX facilities became available, washing machines were on hand, and personnel sometimes got a day off to go to the beach or "safe" areas in Santo Domingo. The work was similar to that at a stateside hospital, except that it was done in fatigue clothing and under tents during the first 6 weeks. During the first few weeks of the operation, mail was dispatched and received three times a week but this was supplemented by package and newspapers brought in on the daily flights from Pope Air Force Base.49
After a few weeks at the airstrip, more suitable quarters for the hospital were found at the Dominican Naval Academy and the hospital was out from under tents (fig. 6). The move was completed just in time to care for the casualties of the mid-June fighting.
39
At the Naval Academy, the hospital usually operated at a 35-to 40-bed capacity (expandable to 100 beds), with its facilities open to civilian emergency cases as well as to any soldier of the IAPF requiring treatment or laboratory work (fig. 7). Hospital personnel also operated a dispensary at the Academy and an additional one at Jaina. The hospital and attached units, except for the helicopter unit, operated in permanent buildings. Helicopter personnel maintained offices under tents on the Naval Academy grounds.
The hospital complex operated in a more or less static situation at the Naval Academy until November, when it was moved 7 miles west of Santo Domingo, on the road to Jaina. There it remained until it was deactivated and the 42d Field Hospital was activated on 10 December 1965. The newly designated unit continued in the same place through the end of the year.
During the year the various medical units on the island operated under the general guidance of the Corps and Division Surgeons and in accordance with their own plans and standing operating procedures to the extent that the situation reasonably allowed. The 307th Medical Battalion and other units also developed new operations plans especially for use in the Dominican Republic. Movement orders were directed by or coordinated with higher headquarters.
After his arrival in the area the Corps Surgeon disseminated medical advice to nonmedical units in the form of USFORDOMREP Medical Bulletin No. 1, dated 12 May 1965 (appendix G). There was no medical appendix to the first command-wide operations order, but the medical appendix to Operations Order 2-65 (appendix H) gathered together the standing policies and
40
Figure 7.-- Ward of the 15th Field Hospital at the Dominican Naval Academy
those lessons learned through experience up to 8 June. This appendix was revised with the subsequent issue of each new operations order. General policies on medical support at the end of the year were spelled out in an unclassified annex to a classified Letter of Instruction to the Commanding General, U.S. Army Forces, Dominican Republic, from the Commanding General, U.S. Continental Army Command, U.S. Army Forces Atlantic Command, Fort Monroe, dated 10 December 1965 (appendix I).
Civil Action Programs
After 3 May, except for the short period of intense fighting in mid-June, most airborne medical activity for the next several months was directed toward civil aid. The 15th Field Hospital opened its hospital and outpatient facilities to all civilians also (fig. 8, map 5). Meanwhile, support to military operations continued in the usual manner.
Civilian casualties were not as serious as they had been described when the whole 15th Field Hospital was rushed to the Dominican Republic, but even before the 82d Airborne Division had fought its way through the center of the city it became obvious that many people were in need of medical help. By 2 May, battle casualties, diseases welling up out of the filth, and the usually inadequate civilian medical capability made less
41
effective when many medical people fled the trouble area, all called for the Army's provision of mass medical assistance. A decision to that effect was made quickly. By 3 May all medical treatment units had their orders and opened their tent flaps to civilians.
The first Civil Medical Assistance Team formed, that of Company D, was typical. It consisted of two medical doctors, two senior aidmen, two interpreters, six ambulance drivers, and assistants. Cases too serious to be handled by the teams were sent back to clearing stations or to the field hospital for hospitalization. Treatment and drugs were offered free.
43
The first day of service rendered by the units was limited to a few handfuls of people because the word had not spread and the local people were hesitant to approach the Americans. But by 8 May people had started flocking to team locations. By that date the 307th Medical Battalion teams had treated 529 persons and delivered two babies. Many of the patients were battle casualties or persons with serious problems. Company B opened a civilian aid facility at an abandoned police station in Santo Domingo and administered to more than 100 people the first day. In the days following, the figure reached 200 to 300 per day (fig. 9).
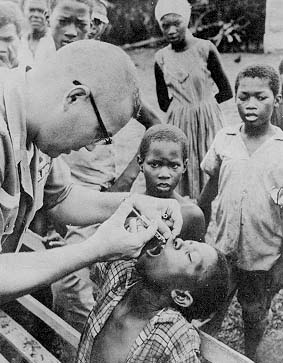
Shortly after the civil aid teams went into action, personnel noticed that many patients' complaints were related to poor dental health. A high number of caries was common among the population because of a lack of care and the high sugar content in the local diet. Therefore, an Army dentist was added to each team.50 His primary function was relieving pain, extracting diseased teeth, and performing emergency care (fig. 10). However, the dentist with Company D at Colegio Maria Auxiliadora performed restorative and reconstructive work for the resident nuns. This was considered partial payment for the work the nuns did, such as doing the laundry without charge, after all the troops moved in.
Women and children made up the greater portion of visitors to aid stations. Malaria, malnutrition, dehydration, vitamin deficiency, worms, tuberculosis, cancer, elephantiasis, yaws, and leprosy, among other things, were observed and treated.
By 10 May, Division medical personnel had seen more than 2,300 patients and were averaging 500 to 600 callers a day. Medical supplies available for civil assistance (including antibiotics and intravenous fluids) were running low. The Corps and Division Surgeons and representatives of the Ministry of Health agreed that most of the extra patient load caused by the revolt had been taken care of and that it was time to get back to civil affairs policy. That is, civil affairs people were to mobilize local professional people and provide them with supplies to care for their own casualties. The XVIII Airborne Corps ordered the assistance stations closed. Signs referring patients to civilian facilities except in extreme emergency were prepared and put up. Although the 15th Field
44
Hospital complied with the policy, the 82d Airborne Division command immediately requested and received permission to continue offering mass civil aid and its stations were reopened. The thinking was that military medical requirements were low and that public relations and American image benefits from civil aid were high.51
Also, the free care had brought some more tangible results. One incidence was the case of a 65-year old man who apparently "paid" for his palliative treatment for cancer by reporting on Communist activity and a plan to smuggle arms across the Ozama River. In several other instances also, "tips" resulted in enlightened tactical intelligence for U.S. Forces.52
45
Right or wrong, the decision to go ahead with the massive civil aid program within the 82d Airborne Division was made and the precedent was set. Also, 10 May could be selected as a date which marked a subtle change in the character of the medical assistance operation. It took on more of the character of a charity program and less of an emergency operation. Many of the ailments treated were of the chronic type and patients tended to be very old or very young. In some instances, where Army physicians were working in close proximity to civilian medical facilities, civilian physicians even referred patients who could not pay to the Army.
And there were a few complaints from local physicians that the Army was ruining their businesses. However, most of the local physicians
46
were glad to have the Army's help since they themselves lacked adequate supplies and facilities, as well as any assurances of safety while conducting their practice.
On 14 May, the Sisters from LaGuardia Church donated drugs to the 82d Airborne Division for use in the civil aid program. Two days later resupply through regular military channels began to arrive. (No medical units ever touched their basic load or any supplies for strictly military use in the civil aid program.)
By the middle of May, 9,369 patients had been cared for, including assistance to casualties from a landslide in Villa Duarte where eight were killed and 12 injured.
Before the end of May many drugs on special order began to become available and treatment of pediatric cases became more effective. More than 24,000 outpatient visits were received before June began.
In June, improved rapport with many local medical facilities resulted in the availability of longer, more definitive care for civilians. The Maternidad Hospital, the Orthopedic Hospital, and the Robert Reid Cabral Pediatric Hospital agreed to receive referrals from U.S. medical teams. Such was not always the case, however. Some of the cooperating civil hospitals would reject maternity cases unable to pay for treatment, so that Army physicians were occasionally called on to perform deliveries on patients who returned and to treat cases of severe dehydration in infants at aid stations.
The civilian patient load dropped off during the June fighting.
Since the 82d Airborne Division did not have the laboratory facilities or medical supplies to handle the chronic type of cases which were becoming more prevalent, the Division tightened its policy somewhat as of 20 June. Thereafter it officially offered treatment only to emergency cases or acutely ill patients. A few aid station teams, at the direction of their combat battalion commanders, continued medical service to all comers throughout the year, but this was the exception rather than the rule. Most civil aid teams in the city continued to function until redeployment, but treated only emergency cases.
The new policy and the return of more and more civilian physicians to the city resulted in a drastic drop in the number of people treated in Santo Domingo. With each passing month the numbers continued to dwindle throughout the year. But by the end of June, Division personnel had reported 39,454 outpatient visits by civilians in the city (fig. 11).
On 28 June, the 82d Airborne Division began a new program under the direction of its Commanding General. The medical companies formed
47
teams which traveled out into the countryside, to small villages such as Parase Estregam, to treat indigent people (fig. 12). The teams would send an advance man into the villages (in the case of Company B. its first sergeant) to seek out the head man, determine the amount of sickness, see if the team would be welcome, and spread the word of its coming. Dysentery and malnutrition were common in the countryside and a wide range of ailments were encountered.
Without question the civil aid programs were the most significant medical activities in the Dominican crisis. The long-range effect of the program will be hard to evaluate, but since the precedent was set, the possible use of mass civil assistance programs will have to be considered in future medical support operations. If they are to be used, programing of necessary supplies into contingency plans will be necessary.
Medical Supplies for Civilian Use
Civil relief supplies for use by civilian agencies represented a large and continuous problem. On 3 May, the Corps Surgeon met with representatives of the Dominican Red Cross, the American Red Cross, the State Department, and the President's emergency aid mission to determine quan-
Figure 12.-- A medical team at a farm approximately 25 miles from San Isidro
tities of medical relief supplies needed.53 A requisition was developed and sent to the United States.
The status of the director of the Dominican Ministry of Health was in doubt at the time and later, so he agreed, as did the conferees, that the Dominican Red Cross, which had a warehouse in a safer location, should act as the single local agency for the control and distribution of the supplies.
In addition to the special requisition mentioned, the 545th Medical Detachment brought in several tons of preplanned civil relief supplies and several Latin American countries contributed food and supplies to the Dominicans.
The Dominican Red Cross processed all the supplies, but the system of distribution was never satisfactory. There were claims that the Red
Cross was discriminatory in its issues, and it appeared to overcontrol supplies. Local hospitals and agencies often found that they could more readily obtain supplies from the U.S. Army than from the Red Cross.
In later weeks the Dominican Red Cross purchased from outside the country supplies which were flown in by U.S. Air Force planes. Several religions organizations also had supplies brought in. Some of the latter were transported by the U.S. Navy.
There were two deficiencies of note in the Army's preplanned relief supplies: few tropical disease medications and almost no pediatric preparations were in the packages.
page updated 19 June 2001
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}